무엇이든 질문하거나 검색하세요...
Hot Research Today
Papers from every journal, all in one place. 맞춤 피드를 만들어 보세요.
가이드라인언급 11회Trending on XExpert Commentary
8월 6일PuriCirculation
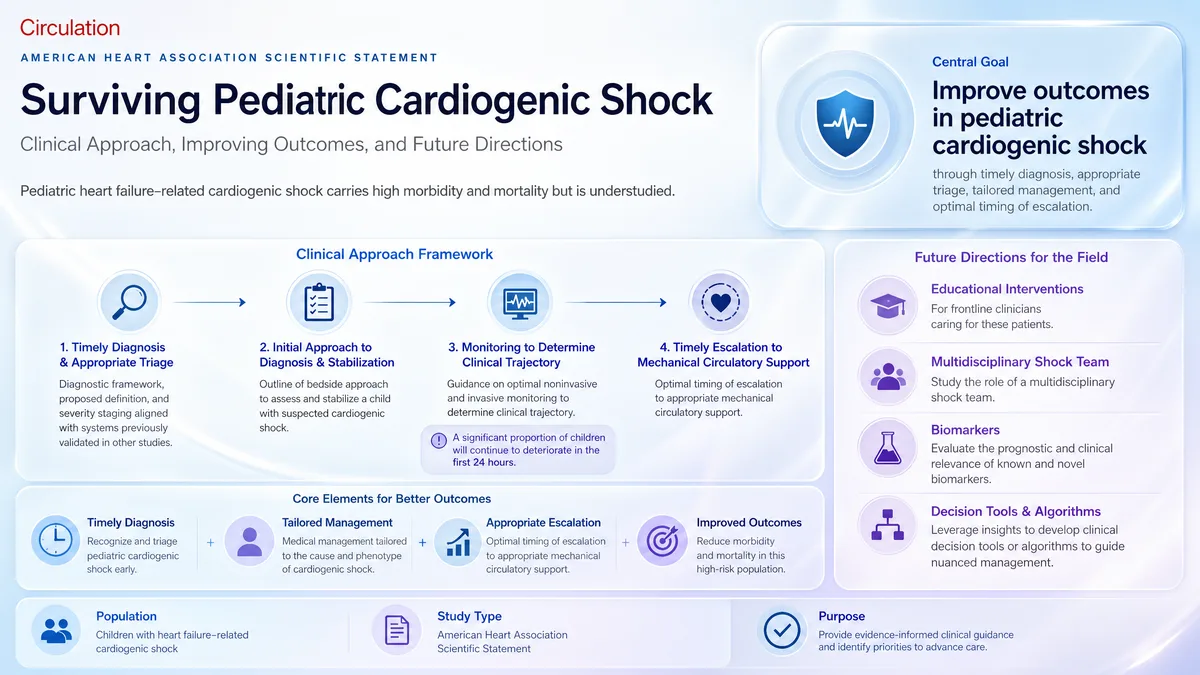
소아 심인성 쇼크 생존: 임상 접근, 결과 개선 및 미래 방향: 미국 심장 협회의 과학적 성명
소아 심인성 쇼크를 위한 진단 프레임워크를 임상의에게 제공; 결과의 전향적 검증을 열어 둠.
meta-analysis · n=13,846언급 8회Expert Commentary
8월 7일ButtCirculation Heart Failure
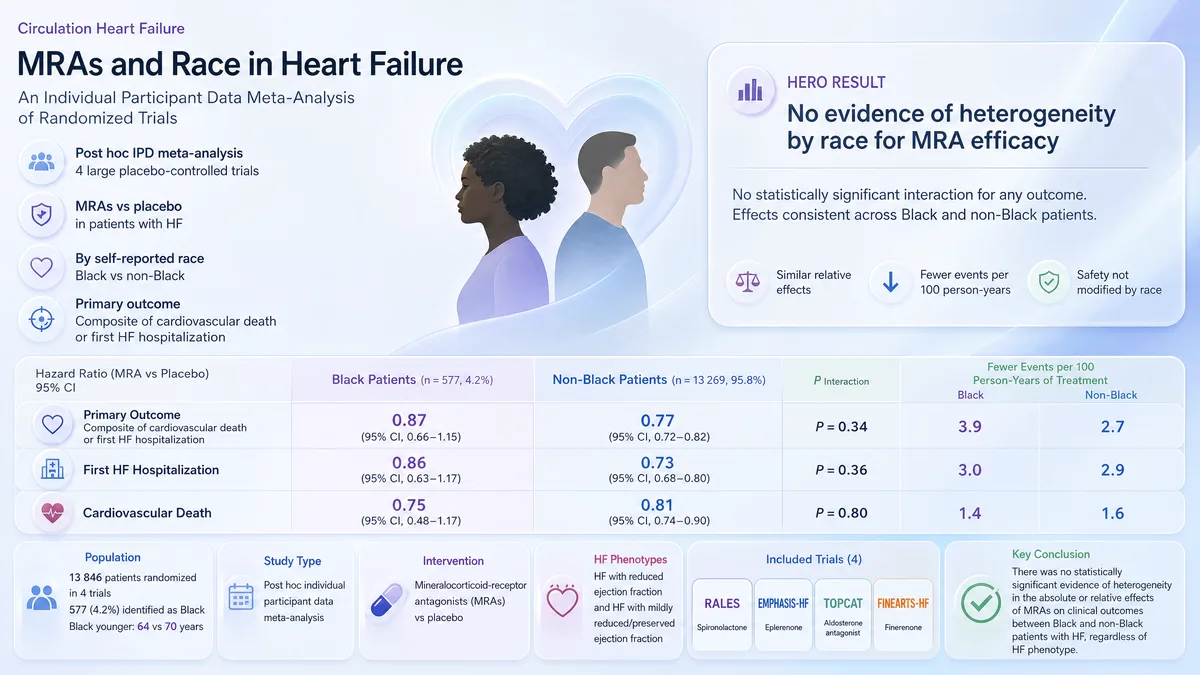
MRAs는 흑인 및 비흑인 환자에서 CV 사망 또는 HF 입원을 유사하게 감소시킵니다.
MRAs는 흑인 및 비흑인 심부전 환자에서 CV 사건을 유사하게 감소시킵니다; 인종 간 일관된 효능을 확인하고 광범위한 사용을 지원합니다.
cohort · n=52,971언급 13회Trending on XExpert Commentary
8월 5일KrügerBMJ
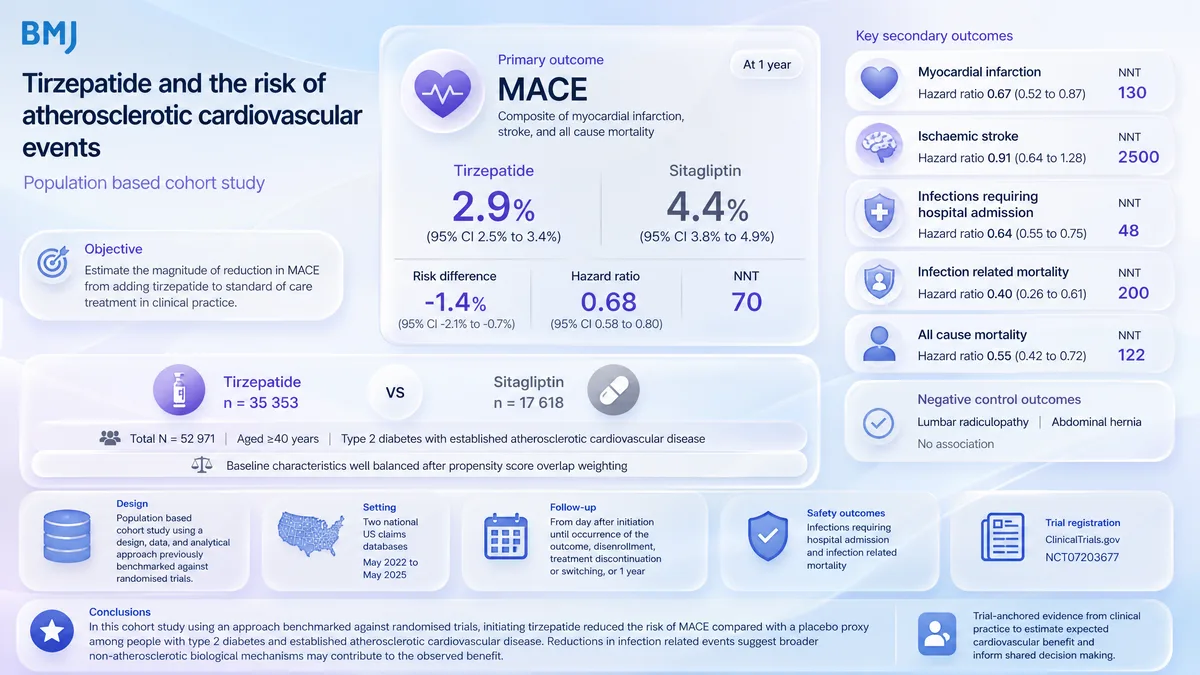
티르제파타이드 시작은 제2형 당뇨병 및 ASCVD에서 시타글립틴 대비 약 32% 낮은 MACE 위험과 관련이 있습니다.
T2D 및 ASCVD에서 티르제파타이드로 MACE 감소를 지원할 수 있으며, 가설 생성에 도움이 되며 RCT의 필요성이 남습니다.
DNDr. Nils Krüger
Resident Physician in the Department of Cardiovascular Diseases, TUM University Hospital
감염에 대한 데이터는 결과가 너무 놀라웠기 때문에 저희를 놀라게 했습니다. 또한, 티르제파타이드로 치료받은 환자 중 병원 입원이 필요한 감염이 상당히 적었습니다: 관련 위험이 36% 감소했습니다. 감염 관련 사망의 위험은 최대 60%까지 감소했습니다.
cohort · n=70언급 6회Expert Commentary
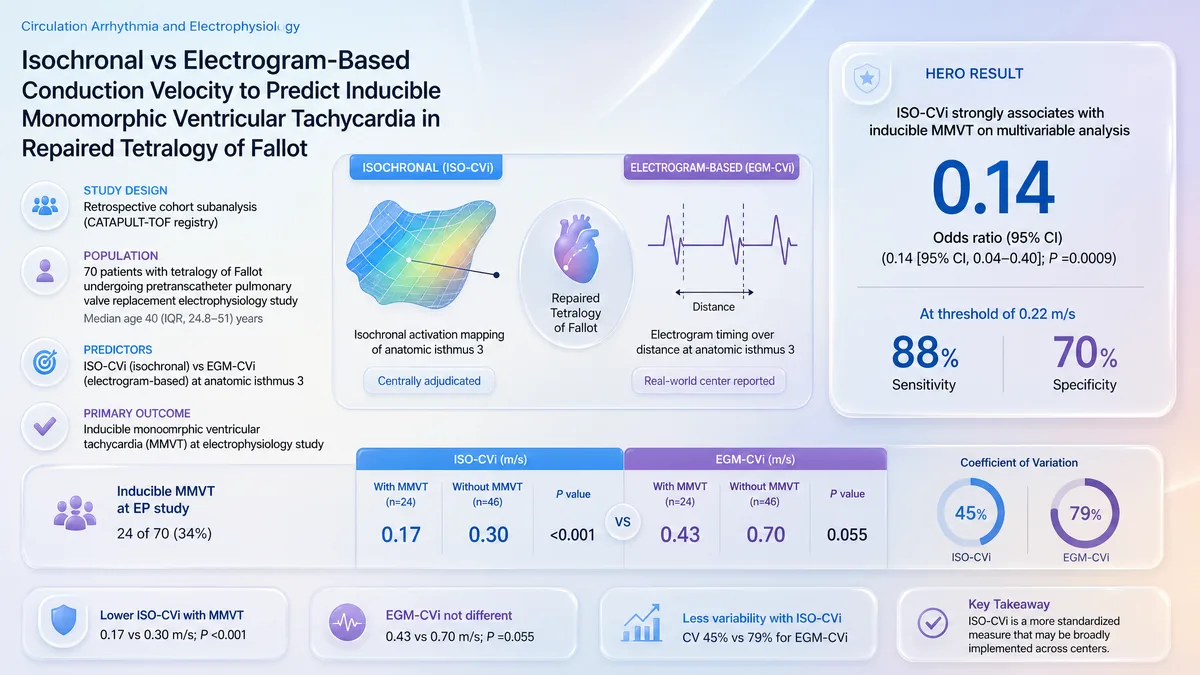
8월 6일O’LearyCirculation Arrhythmia and Electrophysiology
ISO-CVi는 유도 가능한 MMVT의 확률을 약 86% 낮추는 것과 관련이 있습니다.
TOF에서 VT 위험 분류를 위한 ISO-CVi 지원을 가능하게 하며, 전향적 검증을 기다리며 EGM-CVi에 대한 우월성을 남겨둡니다.
cohort · n=273,921언급 15회Trending on XTrending on X
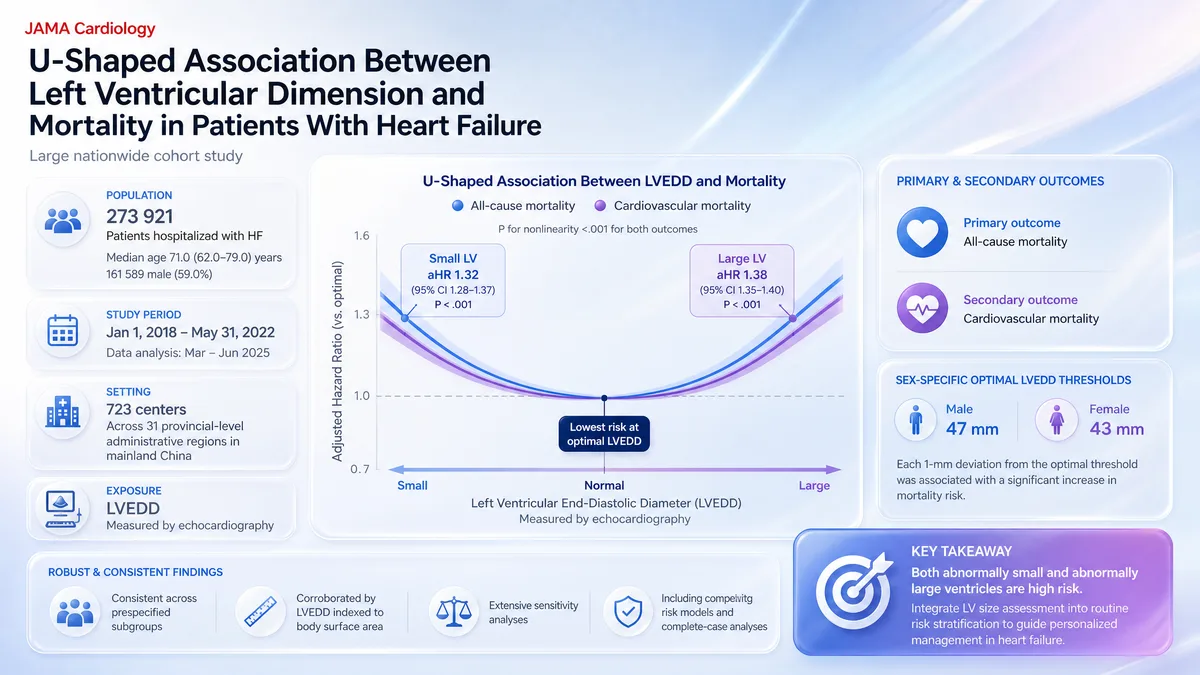
8월 5일WangJAMA Cardiology
작고 큰 LV 크기 모두 HF에서 ~32% 높은 사망률과 연관되어 있습니다.
LV 크기는 LVEF를 넘어 심부전 사망 위험 계층화를 개선할 수 있으며, 치료를 안내해야 하는지는 여전히 열려 있습니다.
DHDr. Hua Wang
Cardiologist, Chinese Cardiovascular Association
LV 크기와 사망률 사이에 U자형 연관성이 나타났다. 비정상적으로 작거나 큰 심실 모두는 독립적으로 모든 원인 및 심혈관 사망률 증가와 관련이 있었으며, 특히 젊은 환자에서 강한 연관성이 관찰되었다. 비정상 LV 또는 수축 기능 장애의 존재는 독립적으로나 조합하여 심부전(HF) 환자에서 사망 위험 증가와 관련이 있었다.
cohort · n=680,864언급 5회Trending on X
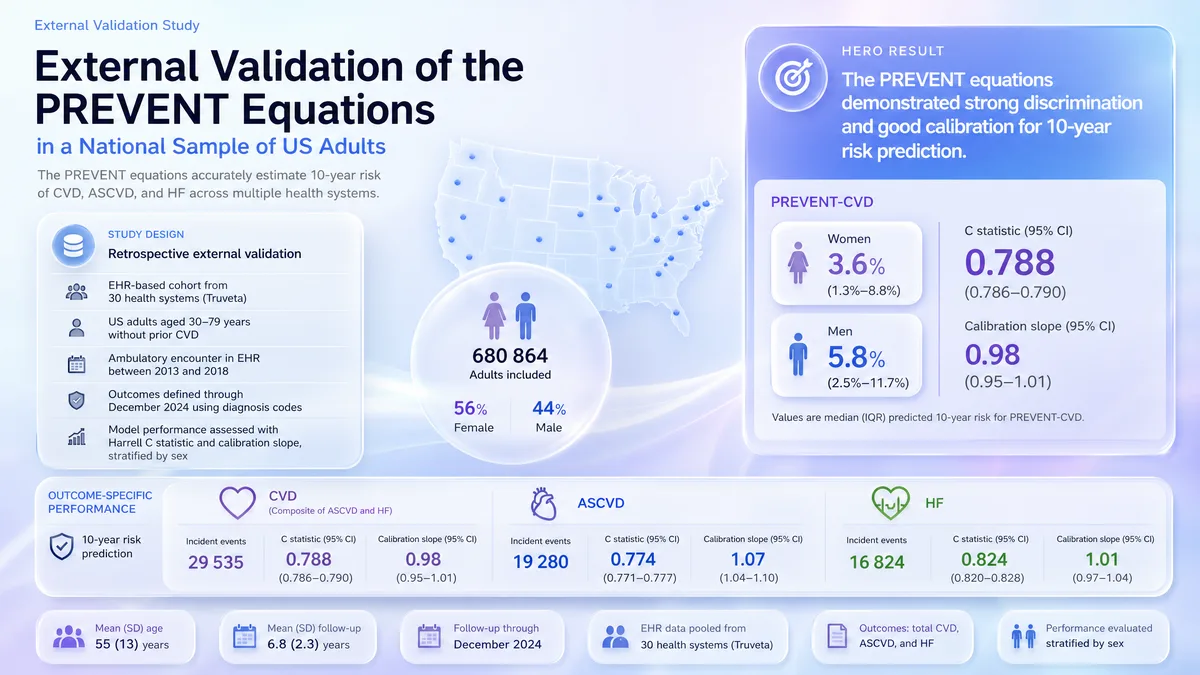
8월 5일KhanCirculation Population Health and Outcomes
PREVENT-CVD는 약 0.79 C-통계량으로 10년 총 CVD 위험을 정확하게 예측합니다.
현재 미국 위험 추정을 위한 PREVENT 사용을 지원하며, 대규모 전자 건강 기록 코호트에 대한 검증을 확장하나, 시험 결과에 따라 채택 여부가 열려 있습니다.
DSDr. Salim S. Virani
Cardiology, Aga Khan University
위험 방정식은 치료 결정이 이루어지는 환경에서 위험을 정확하게 추정하는 한에서만 유용합니다. 이들의 진짜 시험은 현대의 이질적인 인구에서의 보정이며, 특히 추정치가 치료를 시작하고, 예후를 전달하며, 예방 자원을 할당하는 데 사용될 때 그렇습니다. 미국 심장 협회 심혈관 질환 사건 위험 예측(PREVENT) 방정식은 이러한 변화하는 환경을 위해 설계되었습니다.
cohort · n=3,965Expert Commentary
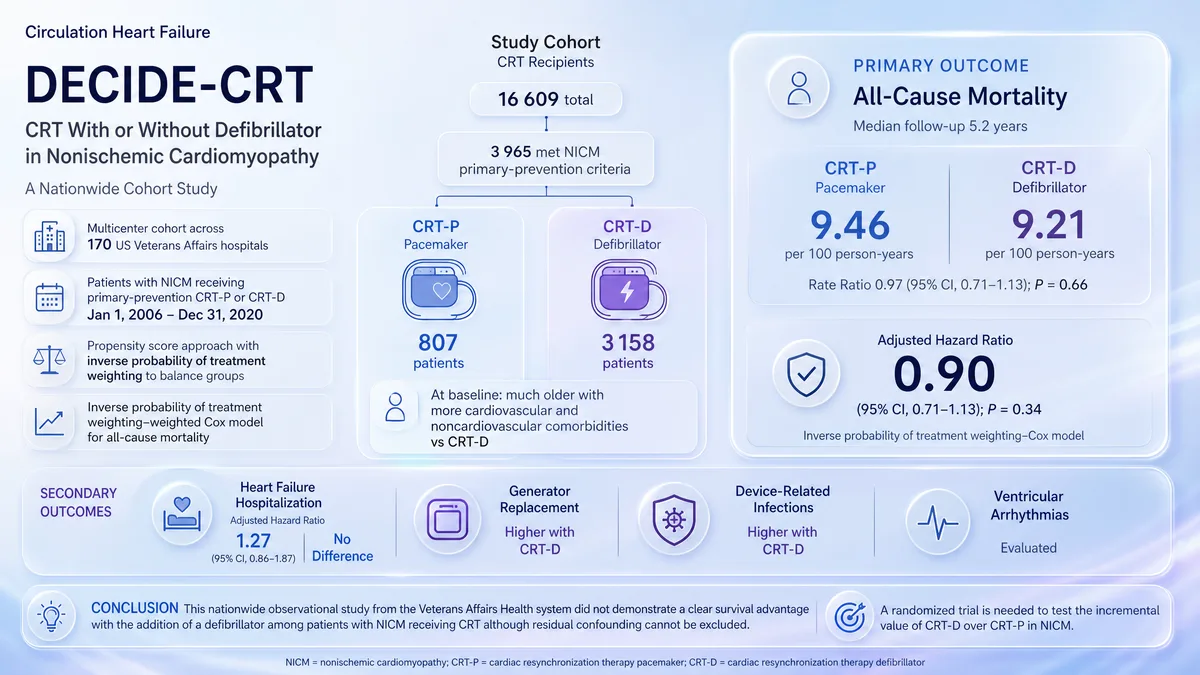
8월 7일SelvaganesanCirculation Heart Failure
CRT-D는 비허혈성 심근병증에서 CRT-P에 비해 장기 생존 이점이 없다.
비허혈성 심근병증에서 CRT-D는 CRT-P보다 낮은 사망률과 관련이 있으며, 제세동기의 이점이 무작위 시험에서 유지되는지는 미지수이다.
cohort · n=202언급 1회Trending on X
8월 10일SongSunhwan'gi
LQT2 및 LQT3 유전자형은 소아 LQTS에서 LQT1에 비해 약 450% 더 높은 생명을 위협하는 부정맥 위험과 연관되어 있습니다.
한국 LQTS 아동의 위험 평가에 정보를 제공할 수 있다; 희박한 아시아 데이터를 확장하지만 일반화 가능성은 열려 있다.
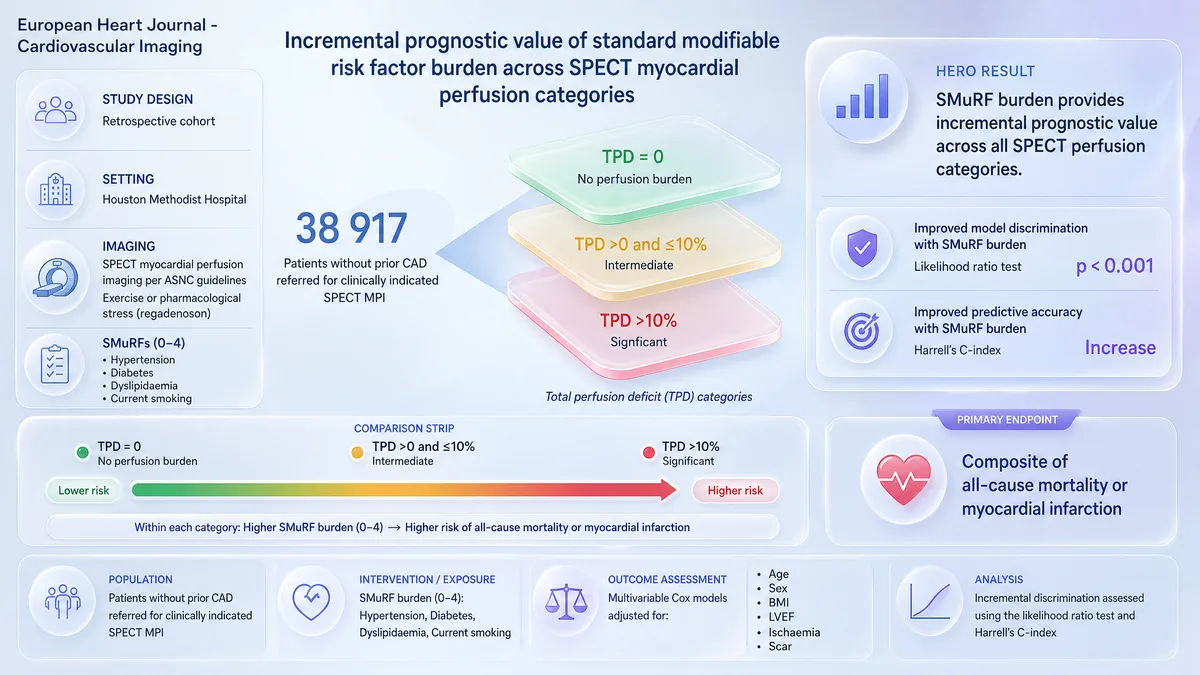
cohort · n=38,917언급 1회
8월 6일GhazawiEuropean Heart Journal - Cardiovascular Imaging
연구는 SPECT 관류 범주에서 SMuRF 부담을 평가하지만 임상 결과 데이터는 보고하지 않음.
SMuRF 부담은 SPECT에서 TPD를 넘어 위험 계층화를 개선할 수 있으며, 임상 관행을 변경하기 전에 전향적 검증의 필요성을 남김.
cohort · n=233
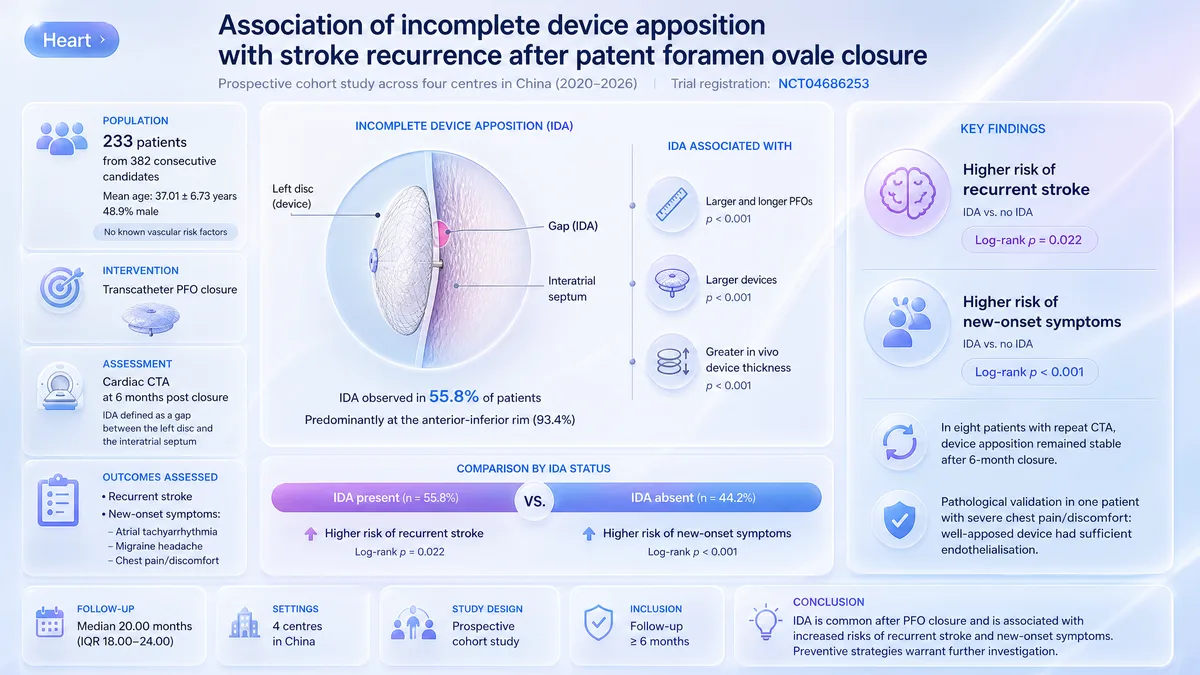
8월 7일YanHeart
PFO 폐쇄 후 불완전한 장치 부착은 재발성 뇌졸중 및 증상에 대한 높은 위험과 연관되어 있습니다.
PFO 폐쇄 후 CTA에서 IDA는 재발성 뇌졸중과 연관되어 있으며, 최적화가 임상 시험에서 사건을 줄이는지 여부는 여전히 불확실합니다.